|
Cardiac Testing Summary of Clinical Indications
|
*Also see our Cardiovascular Diseases Frequently Asked Questions
|
|

Home > For Doctors > Cardiac Testing Summary of Clinical Indications
Exercise Stress Test
- Evaluating the patient with chest pain or with other findings suggestive, but not diagnostic of coronary disease.
- Determining prognosis and severity of disease.
- Evaluating the effects of medical and surgical therapy.
- Screening for latent coronary disease.
- Evaluation of congestive heart failure.
- Evaluation of arrhythmias.
- Evaluation of functional capacity and formulation of an exercise prescription.
- Evaluation of congenital heart disease.
- Stimulus to a change in lifestyle.
In some circumstances the exercise ECG is not useful for diagnosis. ST segment changes on the resting ECG, left bundle branch block, pre-excitation (WPW), and LVH make the exercise ECG uninterruptible for ischemia but don't interfere with assessment of exercise capacity or some parameters used to assess prognosis. Digitalis and tricyclic antidepressants can cause ST depression in the absence of coronary disease. In these situations stress imaging tests such as stress nuclear perfusion studies are indicated.
|
 |
|
|
Cardiac Testing Summary of Clinical Indications
|
*Also see our Cardiovascular Diseases Frequently Asked Questions
| |
Electrocardiogram (ECG or EKG)
In patients with known Cardiovascular Disease or who are at increased risk of developing Cardiovascular Disease:
1) Baseline or initial evaluation
- May disclose useful information regarding diagnosis and prognosis and may permit rational decisions regarding management, including risk of medical and surgical intervention.
- Gives useful information regarding the presence or absence of arrhythmias, conduction defects, chamber enlargement, myocardial hypertrophy, myocardial ischemia, myocardial necrosis, pericardial inflammation and electrolyte disturbance.
2) Response to Therapy
- Conditions in which serial ECGs may be useful include: regression or progression of chamber enlargement or myocardial hypertrophy, resolution or alterations of arrhythmias or conduction disturbances, pacemaker function, acute myocardial infarction or ischemia, electrolyte disturbances, pericarditis, endocarditis, myocarditis, acquired immune deficiency syndrome, transplant rejection, infiltrative cardiomyopathies, therapy with antineoplastic agents and other conditions known to produce ECG changes.
3) Follow-up
- Many cardiovascular diseases undergo progressive worsening with time despite therapy and this progression may be evaluated by periodic ECGs.
4) Before Surgery
- A recent preoperative ECG is recommended in patients with known cardiovascular disease undergoing cardiac or noncardiac surgery.
ECG in patients with no apparent or suspected Cardiovascular Disease:
1) Baseline
- To evaluate persons >40 years of age undergoing physical examination.
- To evaluate patients before administration of pharmacologic agents that are known to have a high incidence of cardiovascular effects.
- To evaluate patients before exercise stress testing.
- To evaluate patients of any age who are in special occupations that require very high cardiovascular performance or whose cardiovascular performance is linked to public safety.
- To evaluate competitive athletes.
2) Response to Therapy
- To evaluate patients in whom prescribed therapy is known to produce cardiovascular effects.
3) Before Surgery
|
|
Cardiac Testing Summary of Clinical Indications
|
*Also see our Cardiovascular Diseases Frequently Asked Questions
|
|
 |
| Holter Monitor |
Holter Monitor
- Palpitations.
- Syncope, presyncope, lightheadedness.
- Antiarrhythmic therapy
- Assessing risk in patients with or without symptoms.
- Myocardial Ischemia.
- Pacemaker function.
- AICD function.
- Heart Rate Variability.
Gated Wall Motion With Ejection Fraction:
- Known or suspected coronary artery disease
- CAD without MI
- Remote MI
- Acute MI
- Known or suspected congestive heart failure (CHF)
- to distinguish ischemic from non-ischemic causes
- to distinguish systolic from diastolic causes
- Evaluation of cardiac function in patients undergoing chemotherapy
- Assessment of ventricular function patients with valvular stenosis and/or insufficiency
Looped Event Recorder:
- Diagnose transient arrhythmias in ambulatory patients.
- Palpitations.
- Syncope, presyncope, light-headedness.
- Antiarrhythmic therapy
- Assessing risk in patients with or without symptoms.
- Myocardial Ischemia.
- Pacemaker function.
- AICD function.
- Heart Rate Variability.
|
|
Cardiac Testing Summary of Clinical Indications
|
|
|
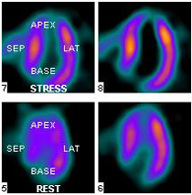
Myocardial Perfusion Imaging: (nuclear stress test)
- Diagnosis of coronary artery disease
- presence
- location (coronary territory)
- extent (number of vascular territories involved)
- Assessment of the degree of coronary stenosis and impact on regional perfusion
- Myocardial Viability Assessment
- ischemia vs. scar
- predict improvement in function following revascularization
- Risk assessment (prognosis) in patients
- post myocardial infarction
- pre-operative work-up prior to major surgery
- Monitoring effect of treatment
- medical therapy for congestive failure or angina
- lifestyle modification
24 Hour Ambulatory Blood Pressure Monitor
- White coat hypertension. With many patients, the physician-patient interaction of the clinic/office environment creates an elevation in blood pressure.
- Diurnal variation. BP is highest during the day and lowest during the night. Once hypertension is identified, physicians can alter, reduce or delete drugs during the normotensive cycle.
- Verification. Confirm office or home measurements.
- Escape from control. ABPM can help identify gaps between antihypertensive medication doses.
- Hypotension. Patients on antihypertensive medication can be monitored to make sure their BP is not reduced to dangerous levels.
- Borderline Hypertension. ABPM provides a bigger picture that may make therapeutic decisions in borderline hypertensive patients easier.
*Also see our Cardiovascular Diseases Frequently Asked Questions
|